
Unfolding Brain-Machine Interfaces: Starting from Basic Science until Neuroprostheses and Neurorehabilitation
UPASHANA CHAKRABORTY
THADOMAL SHAHANI ENGINEERING COLLEGE
upashanachakraborty2014@gmail.com
Brain-Machine Interface and its history:
A brain-machine interface (BMI) is an appliance that interprets neuronal data into instructions provided for controlling external programming or equipment like a computer or automated arm. BMIs are regularly utilized as aided living appliances for humankind with motor or tactile disabilities.
The historical backdrop of BMI begins with Hans Berger’s revelation of the electrical movement of the human brain and the improvement of electroencephalography (EEG). In 1924 Berger was quick to record human brain action through EEG. Studies in the 2010s proposed the expected capacity of neural incitement to re-establish utilitarian connectively. In December 2010, cochlear inserts had been embedded as a Neuroprosthetics appliance in roughly 220,000 individuals worldwide. The first Neuroprosthetics appliance, notwithstanding, was the pacemaker. Neuroprosthetics and BMIs try to accomplish similar points, for example, re-establishing sight, hearing, development, capacity to convey, and surprisingly psychological capacity.
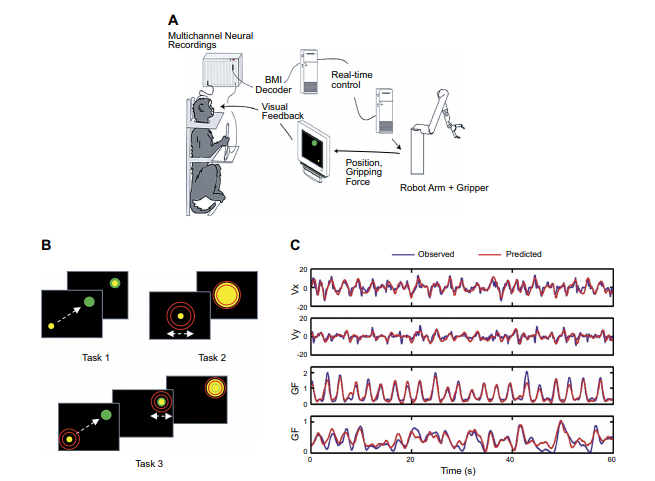
Fig 1: The primary brain-machine interface for coming to and getting a handle on. A: Diagram of the trial arrangement. The extracellular electrical action of neuronal troupes was at the same time recorded from various cortical regions and afterward coordinated to a robotic arm that performed coming to and getting a handle on developments. B: schematics of three engine errands. In task 1, the monkeys put the cursor over a visual objective. In task 2, the joystick was in a fixed position, and the monkeys got a handle on a virtual item by crushing the joystick handle. In task 3, the monkey set the cursor over the objective at that point and created a holding power. C: chronicles of engine boundaries (blue lines) and their translating (red lines). Start to finish: Examples hints of hand speed (Vx, Vy) and grasping power (GF).
BMI for comprehensive Whole-Body Navigation (Neuroprostheses):
The wheelchair is the principal device to help route in individuals with engine inabilities, especially those experiencing serious instances of body loss of motion. One plan for an intracranial BMI that controls wheelchair developments depends on joystick development. They utilized the joystick to consistently control the development of an outside wheelchair. This control was additionally acted in BMI mode, where the wheelchair arrangements were separated from cortical neuronal gatherings. In the BMI tests directed, the monkeys kept on helping developers with the joystick, in the others, the joystick was eliminated and the monkeys controlled the wheelchair without delivering unmistakable arm developments. It depicted how one monkey situated in a wheelchair was prepared to move a joystick in one of four bearings to set the heading of wheelchair development. Under BMI control, this monkey kept on moving the joystick, yet the control signal was gotten from a discrete classifier that separated joystick position from cortical movement. Furthermore, neural control of arm developments may be a futile delegate to empower wheelchair routes. Here it is conjectured that kinematics of entire body developments could be separated straightforwardly from sensorimotor cortical outfits, and used to control a BMI for wheelchair control.
BMI as a prospective Neurorehabilitation Therapy:
Noninvasive BMIs have been utilized as neurorehabilitation devices basically in clinical examinations zeroed in on stroke casualties. The fundamental presumption propelling these investigations has been that training with a BMI that mirrors developments of an impaired appendage could work with cerebrum versatility and add to some even out-of-engine recuperation.
Regardless of being totally paraplegic, stable from the level of the spinal rope injury down, injuries going from (T4-T11), since the day of their spinal line injuries (3–13 years sooner), and coming up short on any physical sensation beneath the level of the injury, after a year time of preparing with this BMI worldview, all patients displayed an extremely critical halfway neurological recuperation, which was described by the accompanying: 1) a normal extension of 5 dermatomes, in pinprick, nonreceptive sensation, in the zone of fractional protection, (underneath the level of the sore); 3) huge improvement in proprioception and vibration discernment beneath the level of the sore; 4) recovery of deliberate control of different muscles beneath the level of the SCI sore, as estimated by EMG chronicles and direct power estimations. Sometimes, patients recovered the capacity to deliver multi-joint leg developments; 6) an improvement in thoracic lumbar control, and 7) rebuilding of peristaltic and defecations, bladder control, and improvement of cardiovascular capacity. Half of the eight patients were updated from complete paraplegia to a halfway paraplegia grouping given this generous neurological recuperation.
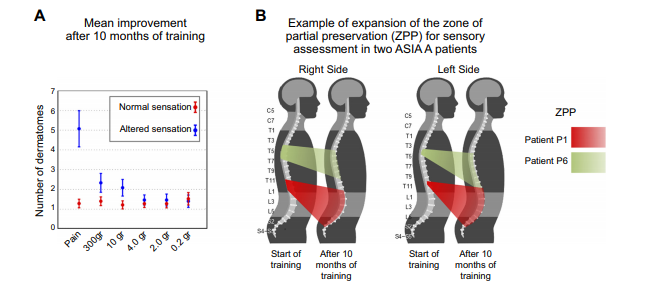
Fig 2: Tactile improvement after neurorehabilitation preparation. A: normal tangible improvement (mean +/- SE by and large patients) following 10 months of preparing. B: illustration of enhancement for Zone of Fractional Safeguarding for tactile assessment for two patients.
Reference (Aug-21-A1)
